Breathless in the Capital
 Air pollution poses serious risks to respiratory health, affecting both individuals with existing conditions and otherwise healthy populations. It leads to bronchoconstriction, respiratory distress, and, lasting health effects including cognitive impairments and behavioural issues. With stricter regulatory measures and mindful actions from the public, improving air quality is achievable—a collective step towards healthier urban living inspired by a simpler, more sustainable lifestyle…
Air pollution poses serious risks to respiratory health, affecting both individuals with existing conditions and otherwise healthy populations. It leads to bronchoconstriction, respiratory distress, and, lasting health effects including cognitive impairments and behavioural issues. With stricter regulatory measures and mindful actions from the public, improving air quality is achievable—a collective step towards healthier urban living inspired by a simpler, more sustainable lifestyle…
By Dr Amitav Banerjee
The quality of the air we breathe is as critical to our health as the water we drink, if not more.
While we can control the water we drink by selecting a reliable source and purifying it to make it potable and safe, we often lack control over the quality of the air we breathe. The safety of drinking water is determined by physical, bacteriological, and chemical parameters, whereas air quality is gauged using certain indicators combined to generate the Air Quality Index (AQI). The AQI measures air pollution levels and assesses its health impact. The higher the AQI value, the poorer the air quality, which can lead to both short- and long-term health issues.

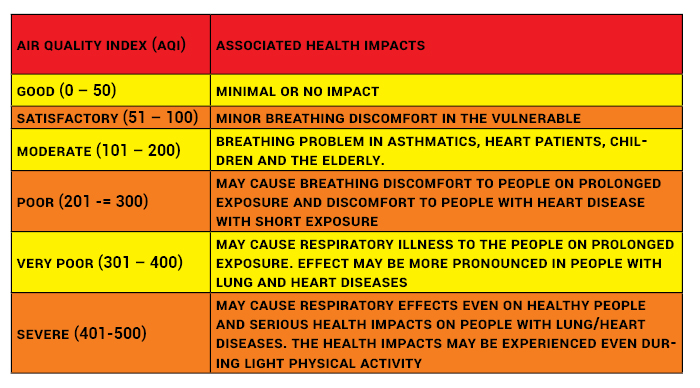
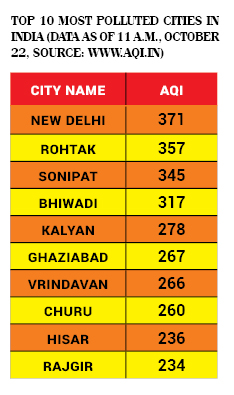
Currently, the overall AQI in Delhi and the surrounding NCR cities ranges from “very unhealthy” to “hazardous” levels. On October 22, Delhi’s AQI was recorded at 371 around 11 am, with several areas across the capital reporting an AQI above 400 in the early hours. An AQI over 300 is considered “very poor,” posing respiratory risks with prolonged exposure, particularly for people with lung and heart conditions. Severe pollution (AQI in the 401-500 range) can trigger respiratory effects even in healthy individuals, along with other health complications.
Air Quality Index: Calculation and Implications
The AQI is an essential tool for monitoring, disseminating information about outdoor air quality, and assessing its impact on public health. The higher the AQI value, the more polluted the air, and the higher the risk of adverse health effects. An AQI value below 50 indicates good air quality—a rare find in urban settings today. In contrast, an AQI above 300 signals hazardous conditions for human health.

Categories and Key Pollutants
The AQI is divided into six categories: Good, Satisfactory, Moderately Polluted, Poor, Very Poor, and Severe. It considers eight primary pollutants, with short-term standards (up to 24 hours) prescribed for each. For an AQI calculation, monitoring data must be available for at least three pollutants, including either PM2.5 or PM10. Particles less than 10 microns (PM10) can be inhaled, presenting grave health risks, while finer particulate matter (PM2.5 or smaller) is even more dangerous due to its ability to penetrate deep into the lungs and bloodstream.
Top 10 Most Polluted Cities in India (Data as of 11 a.m., October 22, Source: www.aqi.in)
Health Implications and Awareness
Raising awareness about the health implications of AQI is crucial for individuals, healthcare practitioners, and civil society. Effective communication about air quality can help motivate stakeholder involvement, guiding public and policy decisions toward cleaner air. The success of air quality initiatives relies heavily on informed citizens who understand local and national air pollution issues and can monitor the progress of mitigation efforts.
To address these issues, AQI information should be presented in a clear, accessible format that simplifies complex scientific and health data. Citizens and policymakers need an effective AQI scale to guide actions to prevent and reduce air pollution, evaluate the impact of interventions, and understand both current and potential future trends in air quality.

Applications of AQI
The AQI serves several purposes:
• Allocating resources and conducting cost-benefit analyses.
• Ranking cities and warning residents and visitors of health hazards.
• Setting and enforcing air quality standards.
• Analyzing historical and current trends for future projections.
• Informing stakeholders, including the public.
• Supporting research on pollution’s health impact and mitigation strategies.
• Prompting political action.
Need for AQI Standardisation
Uniform AQI standards are essential. Without proper standardisation, multiple agencies might report varying AQIs, leading to inconsistencies, such as one agency rating air quality as “good” while another labels it “poor.” Ensuring uniformity in AQI calculations across agencies will allow for a reliable, nationally relevant AQI that accurately reflects the impact of each significant pollutant.
AQI Evolution and Ongoing Development
The concept of the AQI has evolved over time as a tool to measure and communicate air pollution levels and assess their impact on public health.
One of the first AQIs was proposed by Green in 1966, calculated by measuring only two pollutants: sulphur dioxide (SO2) and the Coefficient of Haze (COH). Named the Green Index, it was limited by its narrow scope, omitting other significant pollutants.
In 1969, Fenstock introduced an AQI to evaluate air pollution in 29 US cities. This index estimated pollutant concentrations based on data about source emissions and local meteorological conditions, serving as an early method for assessing pollution potential across metropolitan areas. However, it was not used for daily air quality reports.
In 1970, Canada implemented the Ontario Air Pollution Index, which also measured SO2 and COH. The index provided continuous pollution monitoring through 24-hour running averages, helping citizens remain aware of air quality.
The Oak Ridge Air Quality Index (ORAQI), introduced in 1971, expanded on previous indices by including five pollutants:
• SO2 (sulphur dioxide)
• NO2 (nitrogen dioxide)
• PM (particulate matter)
• CO (carbon monoxide)
• Photochemical oxidants
While ORAQI covered more pollutants, it did not attempt to correlate data with health impacts. The complex calculations and ambiguities of this index also limited its practical application.
The Greater Vancouver AQI (GVAQI) drew upon Canadian federal objectives aimed at protecting both public health and the environment. This index included pollutants such as SO2, NO2, O2 (ozone), total suspended particulates (TSP), COH, and PM10.

Current AQI Efforts in India
In India, AQI development and use have been limited, primarily because the National Air Quality Monitoring Programme began only in 1984. Although the National Environmental Engineering Research Institute (NEERI) in Nagpur started monitoring air quality in 10 cities in 1978, and the Bombay (Now Brihanmumbai) Municipal Corporation began even earlier, AQI was not initially used for public awareness or data interpretation.A recent AQI-related initiative in India is SAFAR (System of Air Quality and Weather Forecasting and Research), which includes air quality forecasting and long-term analysis of pollutant data. However, this study only considered health data from two cities (Delhi and Chennai). Ideally, a countrywide AQI should integrate data from more regions to better represent national air quality.
The Indian Air Quality Index (IND-AQI)
India has now implemented the Indian National Air Quality Standards (INAQS) for 12 parameters, including CO, NO2, SO2, PM10, and PM2.5, O2, lead (Pb), ammonia (NH2), benzo[a]pyrene (BaP), benzene (C2H2), arsenic (As), and nickel (Ni). The first eight parameters have both short-term (1/8/24-hour) and annual standards (except CO and O2), while the remaining four have only annual standards. Both PM10 and PM2.5 are significant due to their specific health risks.
Airborne particulate matter (PM) is a complex mixture of small liquid droplets, solid fragments, and solid cores with liquid coatings. These particles vary in size, shape, and chemical composition and may contain inorganic ions, metals, carbon compounds, and earth-derived elements. For air quality regulation, particles are classified by diameter, with PM10 (10 microns or smaller) being inhalable and potentially harmful. Finer PM2.5 particles are more dangerous due to their ability to penetrate deeper into the respiratory system. The World Health Organization (WHO) suggests no safe threshold for PM concentration below which adverse health effects do not occur.
Health Impact of Ozone
Ozone, a secondary pollutant, has severe health impacts. As a strong oxidant, it can react with many biological materials and cellular components. Exposure to ozone can aggravate conditions like bronchitis, heart disease, emphysema, and asthma, and reduce lung capacity. Common effects include respiratory irritation, coughing, and chest discomfort. Ozone exposure can increase sensitivity to allergens, which are common asthma triggers, leading to aggravated symptoms. It can also cause lung cell inflammation and damage, which the body tries to repair by shedding damaged cells. Ozone exposure may also weaken the immune system, making it harder for the body to fight bacterial infections in the respiratory tract.
Health Impact of Sulphur Dioxide
SO2 is soluble in aqueous media and affects mucous membranes of the nose and upper respiratory tract. A reduction in mean lung function values among groups of healthy individuals has been observed for 10-minute exposures. Asthmatic people appear to respond in a similar way to normal subjects, with the development of bronchoconstriction, but at lower concentrations. Several studies have shown fairly large changes in mean values of lung function indices.
Ammonia and Lead and Their Impact on Health
It is to be noted that most countries have included only six pollutants (described above) in the formulation of the AQI. An attempt has been made to propose breakpoints for NH2 and Pb as these two pollutants also have short-term 24-hour standards. While NH2 can be measured on a continuous basis and can be included in the list of real-time parameters for the AQI, such measurements are not possible for Pb. However, Pb levels can be used in the calculation of the AQI for past days to assess the impact of lead pollution.
Inhalation of high levels of NH2 causes irritation to the nose, throat, and respiratory tract. Increased inhalation may result in coughing, an increased respiratory rate, and respiratory distress. An association has been reported between exposure to ammonia and symptoms like cough, phlegm, wheezing, and asthma at high concentrations.
Lead is a toxic metal, and exposure through all routes results in increased blood lead levels. At lower concentrations, blood lead levels are proportional to air concentration (after accounting for all exposure routes). Lead toxicity can cause anaemia, intestinal colic, and can affect the central nervous system, leading to intellectual disability and behavioural disorders. Urgent action is called for when the AQI is very poor or severe. This includes actions by regulatory bodies as well as the public.
Actions to Be Taken by Regulatory Agencies
The regulatory bodies should establish the sources of emissions responsible for very poor or severe AQI levels. Necessary steps must be taken to further regulate the emissions that are significantly impacting ambient air quality. Specific actions may include:
• Strict vigilance and zero tolerance for visible polluting vehicles, industries, open burning, construction activities, etc.
• Regulating traffic.
• Identifying sources that significantly contribute to rising air pollution levels and taking action to reduce emissions from these sources.
Actions to Be Taken by Citizens
• Maintain vehicles properly (e.g., get PUC checks, replace air filters, and maintain correct tyre pressure).
• Follow lane discipline and speed limits, avoid prolonged idling, and turn off engines at red traffic signals.
• During severe or very poor AQI categories, people should minimise travel, avoid using private vehicles, use public transport, walk or bike, and carpool.
• Use smaller vehicles (e.g., avoid SUVs).
• Minimise the use of diesel generators.
• People, especially those with heart disease or asthma, should consider avoiding unnecessary exposure.
Long-term Strategies to Improve AQI
Major paradigm shifts are needed to address the problems of air pollution and associated health issues. Mahatma Gandhi expressed concerns about urbanisation and mechanisation and their environmental impact. He warned that abolishing cottage industries would eliminate employment opportunities in rural areas and promote urban migration. He emphasised production by rural masses over mass production in urban areas. Adopting aspects of Gandhi’s lifestyle of austerity can improve both air quality in cities and public health. Automobiles pollute the atmosphere and also promote sedentary habits, leading to obesity and chronic diseases. Market forces that promote new cars on already congested Indian roads and ultra-processed foods for the sedentary urban middle class contribute to the poor quality of air and food.
Gustavo Petro, former mayor of Bogota, once said, “A developed country is not a place where the poor have cars. It is where the rich use public transport.” Fast-developing economies like India should pause and introspect. Adopting the vision and lifestyle of Mahatma Gandhi, even partly, by both society and individuals can address some of the problems of urban air pollution.
(The Author is a renowned epidemiologist, currently Professor Emeritus at DY Patil Medical College, Pune)